SOTYKTU SELECTIVELY TARGETS TYK2, A KEY LINK IN THE IL-23/IL-17 INFLAMMATORY PATHWAY1-3

SOTYKTU is an oral, small-molecule TYK2 inhibitor that works intracellularly

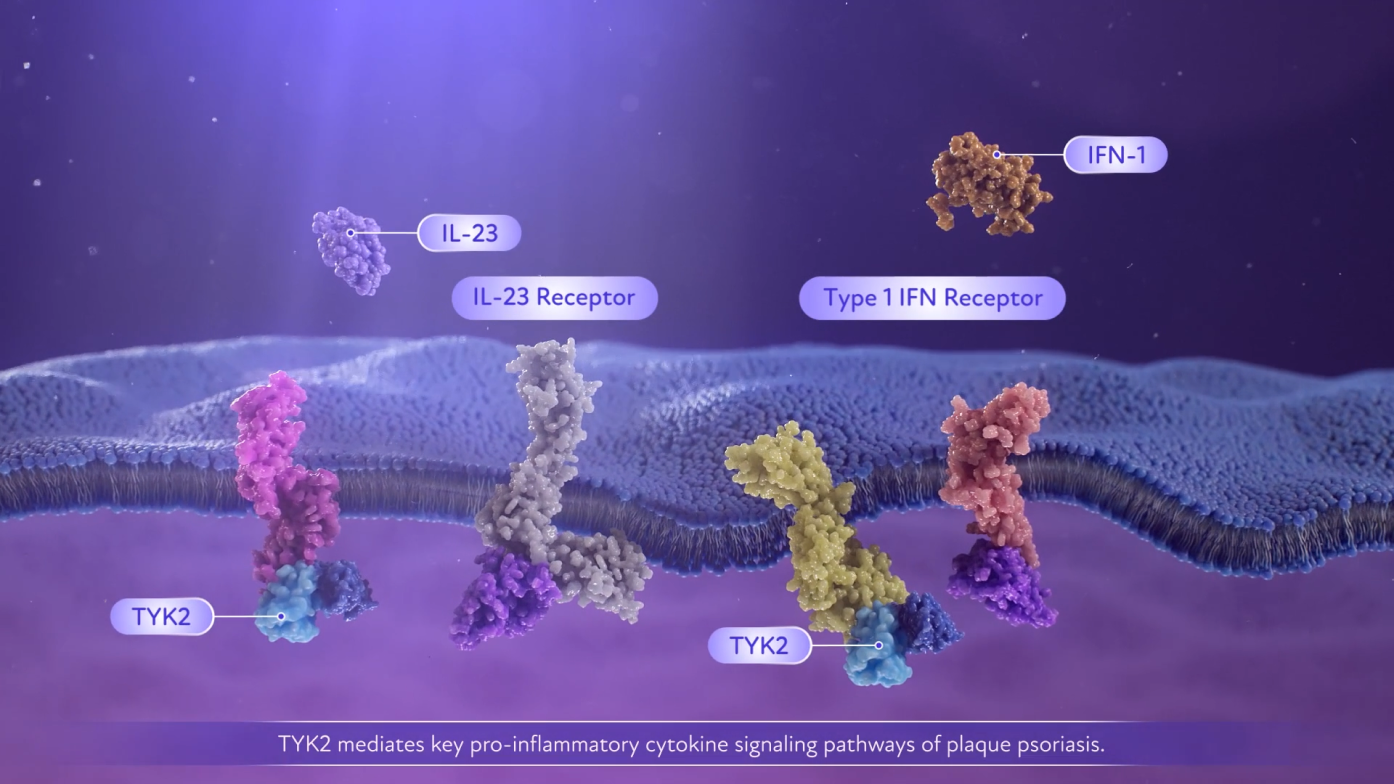
- TYK2 mediates multiple cytokine pathways, including IL-23, IL-12, and Type I IFN1-3
- TYK2 is an important link between IL-23 and IL-17, key inflammatory cytokines in psoriasis1,3
The precise mechanism linking inhibition of TYK2 enzyme to the treatment of moderate-to-severe plaque PsO or active PsA is not currently known.1
| Tyrosine kinase 2 is a member of the Janus kinase family.1 TYK2 pairs with JAK1 or JAK2 to mediate multiple cytokine pathways and transmit signals.1 |
| * | SOTYKTU reduced psoriatic-related gene expression in psoriatic skin in a dose-dependent manner, including reductions in IL-23-pathway and Type I IFN-regulated genes.1 |
| † | SOTYKTU reduced IL-17A, IL-19, and beta defensin following 16 weeks of treatment. The relationship between these pharmacodynamic markers and the mechanism(s) by which SOTYKTU exerts its clinical effects is unknown.1 |
| ACR=American College of Rheumatology; IFN=interferon; IL=interleukin; JAK=Janus kinase; PsA=psoriatic arthritis; PsO=psoriasis; STAT=signal transducer and activator of transcription; Th17 cell=T helper 17 cell; TYK2=tyrosine kinase 2. |
SELECT IMPORTANT SAFETY INFORMATION
Potential Risks Related to JAK Inhibition: It is not known whether tyrosine kinase 2 (TYK2) inhibition may be associated with the observed or potential adverse reactions of Janus Kinase (JAK) inhibition. In a large, randomized, postmarketing safety trial of a JAK inhibitor in rheumatoid arthritis (RA), patients 50 years of age and older with at least one cardiovascular risk factor, higher rates of all-cause mortality, including sudden cardiovascular death, major adverse cardiovascular events, overall thrombosis, deep venous thrombosis, pulmonary embolism, and malignancies (excluding non-melanoma skin cancer) were observed in patients treated with the JAK inhibitor compared to those treated with TNF blockers. SOTYKTU is not approved for use in RA.
PLEASE SEE ADDITIONAL IMPORTANT SAFETY INFORMATION BELOW.
Take a closer look at the SOTYKTU MOA
Watch videos to learn about the SOTYKTU MOA.
ARE YOU READY TO EXPLORE MORE? SELECT A TOPIC BELOW.
References:
- SOTYKTU [package insert]. Princeton, NJ: Bristol-Myers Squibb Company; 2026.
- Chimalakonda A, Burke J, Cheng L, et al. Selectivity profile of the tyrosine kinase 2 inhibitor deucravacitinib compared with Janus kinase 1/2/3 inhibitors. Dermatol Ther (Heidelb). 2021;11(5):1763-1776. doi:10.1007/s13555-021-00596-8
- Di Cesare A, Di Meglio P, Nestle FO. The IL-23/Th17 axis in the immunopathogenesis of psoriasis. J Invest Dermatol. 2009:129(6):1339-1350. doi:10.1038/jid.2009.59